Hot flashes, night sweats, mood swings. These get all the attention when we talk about menopause. But there’s another change that quietly affects roughly halfof women going through this transition, and many suffer through it in silence: thinning hair, loss of volume, changes in texture, a part that keeps getting wider.
For decades thestory was simple. Estrogen falls, hair thins. Use the same shampoo, maybe try a thickening conditioner, hope for the best.
That story is being rewritten. A wave of recent research suggests midlife hair loss isn’t just a hormone problem. It’s an inflammation problem, a microbiome problem, an energy problem, and a barrier problem, all happening at the same time, in the same square inches of skin you’ve been treating like a hair-styling surface for decades. The most interesting question being asked in the field right now is whether the hair follicle itself can go through a kind of “menopause” even in women whose ovaries are still working perfectly fine.
Here’s what the current science actually says, and wh
y it changes how you should think about caring for your hair after 40.
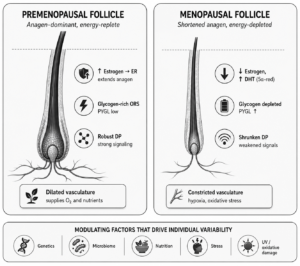
Figure 1. Comparison of a premenopausal hair follicle (left) with a follicle in the menopausal transition (right). Hormonal shift, depleted glycogen reserves, shrinking dermal papilla and constricted vasculature combine with modulating factors (genetics, microbiome, nutrition, stress and oxidative damage) to produce individual variability in midlife hair changes.
The follicle as a metabolically expensive mini-organ
Start with the original provocation, from Rinaldi and colleagues at Milan’s Human Microbiome Advanced Project (Biomedicines, 2023). They make a few points that reframe the whole conversation.
Producing a single gram of hair requires roughly 670 kilojoules of energy, comparable to six minutes of vigorous exercise. Multiply that by the ~100,000 follicles on your scalp and you start to see why hair is one of the most metabolically demanding tissues in the body. To support that, follicles run primarily on aerobic glycolysis and operate their own internal Cori cycle, storing glycogen in the outer root sheath and breaking it down on demand via an enzyme called glycogen phosphorylase (PYGL).
Estrogen helps that energy economy in two ways. It binds to estrogen receptors in the dermal papilla and extends the anagen (active growth) phase of the hair cycle. It also acts as a vasodilator, keeping blood vessels in the scalp open so oxygen and nutrients reach those hungry follicles.
When estrogen falls at menopause, both supports weaken. Anagen shortens, vessels constrict, and the follicle has less of what it needs to produce a thick, pigmented hair shaft. Combine that with a slightly higher relative androgen-to-estrogen ratio (because absolute androgen levels in women fall more slowly than estrogen), and you get the classic female-pattern picture: a widening part, miniaturized hairs, diffuse thinning across the crown.
But here is the bit Rinaldi’s group flags as most interesting. In their dermatology practice they’ve identified women aged 35 to 55 with no hormonal markers of menopause and no menopausal symptoms, yet 12% of them showed female-pattern hair loss with thinning and miniaturization. The histology didn’t fit androgenetic alopecia or telogen effluvium. Their hypothesis: there may be a hair follicle “menopause” that’s clinically independent of systemic menopause, driven by changes in the follicle’s metabolism, estrogen receptor responsiveness, genetics, and the scalp microbiome.
So if it’s not just estrogen, what else is going on?
Hair loss has an inflammation problem
For decades, female-pattern (and male-pattern) hair loss was classified as “non-inflammatory.” That label is now considered outdated.
The shift began with David Whiting’s seminal 1993 histology study, which found perifollicular lymphocytic inflammation in roughly 40% of androgenetic alopecia biopsies. Two decades later, Ramos and colleagues (2016) showed that this inflammation isn’t just incidental. It’s specifically associated with apoptosis (programmed cell death) in miniaturizing follicles in women with female pattern hair loss. Plante et al. (2020), reviewing modern AGA biopsies at the Medical University of South Carolina, confirmed the same finding: perifollicular inflammation and follicular spongiosis are commonly present in pattern hair loss.
What does the inflammation actually do? Yoo and colleagues (2006) provided a mechanistic answer. Testosterone treatment of human scalp dermal fibroblasts increased TGF-β1 and type I procollagen (the molecular signatures of fibrosis), and finasteride blocked it. So DHT doesn’t just shrink follicles; it triggers fibrotic scarring around them, slowly choking off the environment a healthy follicle needs.
The most striking evidence that this inflammatory pathway can run independently of hormones comes from postmenopausal frontal fibrosing alopecia (FFA), first described by Kossard in 1994. These women showed progressive frontal hairline recession with dense perifollicular fibrosis and activated T-helper cell infiltrates around the follicles. Crucially, their androgen levels were not elevated. Something other than DHT excess was driving the immune attack on the follicle.
This is why dermatologists no longer think of pattern hair loss as a purely hormonal-mechanical process. It’s increasingly understood as a low-grade inflammatory condition that the hormonal shift of menopause can amplify but doesn’t fully explain.
Inflammaging, senescence, and a scalp that’s older than it looks
The newest piece of the puzzle is the recognition that the scalp itself is undergoing accelerated cellular aging during the menopausal transition, and that aging generates inflammation as a byproduct.
Westgate, Grohmann and Sáez Moya (J Clin Med, 2025) brought this together in a comprehensive review titled Hair Longevity. Their core argument: many of the same processes driving aging in other tissues are happening in the scalp, and they matter for hair.
- Cellular senescence and SASP. Aged scalp cells stop dividing but don’t die. Instead, they enter a “senescent” state and begin secreting a cocktail of inflammatory cytokines and damage-signaling molecules, the senescence-associated secretory phenotype (SASP). The result is chronic, sterile, low-grade inflammation around the follicle, even without infection or injury.
- Endothelial cell senescence in scalp blood vessels reduces their ability to deliver nutrients to follicles. This compounds the vasoconstriction caused by estrogen loss.
- Reactive oxygen species generated by mitochondria, UV exposure, pollution, and microbial dysbiosis amplify this microinflammation.
- Mitochondrial decline in scalp tissue reduces ATP production exactly when follicles need more energy to maintain anagen.
Williams and colleagues (2021) provided some of the underlying evidence by showing that the female scalp dermal sheath and dermal fibroblasts change measurably with age, altering the structural and biochemical environment that follicles depend on.
This is what “inflammaging” looks like at the level of the scalp. It’s not a dramatic, visible inflammation. It’s a quiet biochemical drizzle of inflammatory signals that most women never notice, until they start finding more hair on their pillow.
When sebum disappears, the microbiome shifts
The scalp is one of the most sebum-rich sites on the human body, and that matters more than people realize. Sebum isn’t just grease. It’s the food source for the resident microbial community that lives on every healthy scalp.
Zouboulis and colleagues, in a widely cited 2022 Climacteric review on menopause and skin, document that sebaceous gland activity declines after menopause, contributing to dryness, accelerated transepidermal water loss, and weakened barrier function. Pagac, Stalder and Campiche (Frontiers in Aging, 2024) directly demonstrated that this sebum decline shifts the skin microbiome composition in postmenopausal women. The same mechanism applies to the scalp, which depends on similar lipid substrates for its microbial inhabitants.
A growing body of microbiome research (Polak-Witka et al., 2020; Lousada et al., 2021) has shown that the scalp and the hair follicle each host distinct microbial communities, and that imbalances in those communities (too much Cutibacterium acnes, too little Staphylococcus epidermidis, shifts in Malassezia species) correlate with hair loss conditions including AGA. The Rinaldi group’s own earlier work (Pinto et al., 2019; 2022) documented bacterial shifts in alopecia areata and lichen planopilaris, supporting the idea that microbial dysbiosis isn’t a passive bystander but an active modifier of follicle health.
So when sebum drops, the microbiome shifts. When the microbiome shifts, it stops doing its protective job. And that contributes to the same low-grade inflammation that’s already being stoked by senescence and hormonal change.
The picture all these paints
Line these papers up next to each other and a coherent picture emerges that’s a long way from “estrogen drops, hair thins”:
- Hormonal shift lowers estrogen, raises the relative androgen ratio, shortens anagen, and constricts scalp blood vessels.
- Cellular senescence in scalp fibroblasts, dermal sheath cells and endothelial cells generates a chronic SASP-driven inflammatory environment around follicles.
- Perifollicular microinflammation and fibrosis become measurable on biopsy in the majority of women with female-pattern hair loss, even those without elevated androgens.
- Sebum production drops, weakening the scalp barrier and depriving the microbiome of its substrate.
- Microbial dysbiosis feeds back into follicular inflammation and oxidative stress.
- Energy supply to the follicle declines with less blood flow, less mitochondrial output, and less glycogen, exactly when the inflammatory environment makes recovery harder.
The follicle is being squeezed at the cellular, hormonal, vascular, microbial, and metabolic levels simultaneously. The visible thinning of your hair is the downstream consequence of all this happening at once.
Why “hair care” stops working, and what comes next
If you accept that picture, the implication is uncomfortable for an industry built on shampoos, conditioners, and styling sprays. Those products are operating on the wrong organ. They’re treating the hair fiber. The action is happening in the skin underneath.
This is exactly the shift Westgate et al. describe in their 2025 review when they talk about the “skinification of hair”. This movement borrows the entire conceptual vocabulary of modern skincare (barrier function, microbiome support, anti-inflammatories, antioxidants, nutrient delivery) and applies it to the scalp.
Because here’s the thing. By your 50s, the scalp you’re styling is biologically more like an aging facial skin than a passive base for hair. It needs:
- Barrier support. The same logic that makes ceramides and niacinamide useful on the face applies to the scalp. A compromised stratum corneum on the scalp itches, flakes, and grows worse hair.
- Microbiome-friendly cleansing. Harsh sulfates that strip remaining sebum make dysbiosis worse. Gentler surfactants, pre/postbiotics, and balanced pH formulas are emerging for exactly this reason.
- Anti-inflammatory actives. Niacinamide, panthenol, piroctone olamine, zinc pyrithione (which calm inflammation in addition to their antimicrobial effects), green tea polyphenols, caffeine, plant flavonoids.
- Antioxidant support to quench the reactive oxygen species feeding the senescence cycle.
- Nutrient delivery, both topical (peptides, adenosine, marine collagen) and systemic (correcting genuine deficiencies in iron, where ferritin under 70 ng/mL is a recognized risk threshold in women, plus vitamin D, protein, possibly zinc).
- Energy and metabolism support. Newer interventions like spermidine supplementation are being investigated for their role in maintaining follicle anagen.
- The fiber itself. Bond-builder technologies repair damage to the existing hair shaft, but that’s a separate problem from the follicle.
No single one of these is a fix. The trend in the evidence is toward layered, individualized regimens that address multiple drivers at once, closer to the way a thoughtful skincare routine targets multiple aspects of facial aging than to the single-product mindset of traditional haircare.
To make this concrete, here is what a formulation built around these principles actually looks like in practice. The Layla & Kays range, developed by the team at HexisLab, layers several of the categories above into a single sulphate-free system designed for textured and sensitised scalps:
- A sulphate-free cleansing base. Built on mild amino acid and sugar-derived surfactants (sodium lauroyl sarcosinate, cocamidopropyl betaine, decyl glucoside, sodium lauroyl methyl isethionate) that clean the scalp without stripping its remaining sebum or disrupting the microbiome.
- Antioxidant actives targeting oxidative stress. Mango leaf extract (a natural source of mangiferin), sodium ferulate (ferulic acid), rice bran extract, prickly pear seed oil and patawa fruit oil all contribute free-radical scavenging activity to the scalp environment.
- Anti-inflammatory and barrier-supporting botanicals. Aloe vera, coconut oil and orange fruit extract help calm low-grade scalp inflammation and reinforce barrier function.
- Amino acids to feed the hair shaft. Wheat and soy amino acids alongside arginine, serine and threonine support keratin structure and resilience.
- Two proprietary HexisLab complexes. MitoTech™ is designed to support cellular energy in the follicle, addressing the metabolic decline discussed earlier. PhytoProtect™ is targeted specifically at oxidative stress in the scalp environment.
- A clean credentials baseline. Sulphate-free, paraben-free, vegan, halal-certified and cruelty-free.
The point isn’t that one product solves midlife hair changes. The point is that an evidence-aligned formulation now looks very different from a 1990s shampoo. It is closer to a piece of skincare designed for a specific biological problem.
What this means in practice
If you’re watching your hair change and feeling like the products on your bathroom shelf aren’t doing what they used to, the literature suggests you’re not imagining it. And you’re probably treating the wrong thing.
A reasonable framework, supported by the evidence above:
- Get a workup. Significant hair loss deserves a dermatology visit. Iron, ferritin, vitamin D, thyroid, and (if relevant) hormonal panels are worth checking. Treat what’s actually deficient.
- Treat your scalp like skin. Cleanse gently. Don’t overuse heat or harsh chemistry. Look for products that mention the scalp barrier, microbiome, and anti-inflammatory actives, not just “volumizing.”
- Feed the follicle from inside. The metabolic argument is real. A diet adequate in protein, iron, zinc, omega-3s and antioxidants gives the follicle the substrates it needs. Chronic under-eating in midlife is a common, under-recognized contributor to hair shedding.
- Don’t ignore stress, sleep, and UV. All three drive oxidative stress and SASP. The same lifestyle measures that slow facial skin aging slow scalp aging too.
- Be patient and consistent. Pattern hair loss treatments typically take 4 to 12 months to show visible benefit. Shedding tends to lessen first, before density visibly improves.
Why these matters
The bigger contribution of the new research isn’t a single new treatment. It’s a new way of thinking. The hair follicle isn’t a passive bystander to hormonal change. It’s a metabolically demanding mini-organ embedded in a piece of skin that is itself aging, changing its microbiome, losing its barrier integrity, and generating its own inflammatory weather.
Once you see midlife hair loss as the convergence of all these forces, the way forward becomes both more humbling and more hopeful. There’s no single magic ingredient. But there’s also no longer any reason to feel that “your hair is just getting older” is a complete explanation, or that there’s nothing meaningful to be done.
Treat the scalp, feed the follicle, calm the inflammation, support the microbiome, and give it time. Your hair has been trying to tell you something. The science is finally catching up.
Help us understand this better
This article reflects what the published science currently says, but the lived experience of women going through these changes is the part the literature still under-represents. We are now running a wider study on this phenomenon, looking at how women experience the convergence of hormonal, inflammatory, microbial and metabolic shifts during the menopausal transition, and how a scalp-first approach affects what they see in the mirror.
If any of this resonated with your own experience, we would love to hear from you. Leave a comment below with your story or email the team directly at info@hexislab.com . Every account helps build a clearer picture of what is happening to women’s hair in midlife, and what helps.
Selected references
- Rinaldi F, Trink A, Mondadori G, Giuliani G, Pinto D. The Menopausal Transition: Is the Hair Follicle “Going through Menopause”? Biomedicines. 2023;11(11):3041. PMID: 38002043.
- Westgate GE, Grohmann D, Sáez Moya M. Hair Longevity: Evidence for a Multifactorial Holistic Approach to Managing Hair Aging Changes. J Clin Med. 2025;14(6):1894. PMID: 40142702.
- Zouboulis CC, Blume-Peytavi U, Kosmadaki M, et al. Skin, hair and beyond: the impact of menopause. Climacteric. 2022;25(5):434-442. PMID: 35377827.
- Kamp E, Ashraf M, Musbahi E, DeGiovanni C. Menopause, skin and common dermatoses. Part 1: hair disorders. Clin Exp Dermatol. 2022;47(12):2110-2116. PMID: 35796569.
- Williams R, Westgate GE, Pawlus AD, Sikkink SK, Thornton MJ. Age-Related Changes in Female Scalp Dermal Sheath and Dermal Fibroblasts. J Invest Dermatol. 2021;141(5):1041-1051. PMID: 33326808.
- Ramos PM, et al. Apoptosis in follicles of individuals with female pattern hair loss is associated with perifollicular microinflammation. Int J Cosmet Sci. 2016. PMID: 27163333.
- Yoo HG, et al. Perifollicular fibrosis: pathogenetic role in androgenetic alopecia. Biol Pharm Bull. 2006. PMID: 16755026.
- Kossard S. Postmenopausal frontal fibrosing alopecia. Scarring alopecia in a pattern distribution. Arch Dermatol. 1994. PMID: 8002649.
- Polak-Witka K, Rudnicka L, Blume-Peytavi U, Vogt A. The Role of the Microbiome in Scalp Hair Follicle Biology and Disease. Exp Dermatol. 2020;29(3):286-294. PMID: 30974503.
- Lousada MB, et al. Exploring the Human Hair Follicle Microbiome. Br J Dermatol. 2021;184(5):802-815. PMID: 32762039.
- Pagac MP, Stalder M, Campiche R. Menopause and facial skin microbiomes: a pilot study revealing novel insights into their relationship. Front Aging. 2024;5:1353082.